
Ankylosing Spondylitis
Inflammatory back pain that starts young, and the third post in our spondyloarthritis series.
This is the third post in our spondyloarthritis series. Today is ankylosing spondylitis, or AS, which is one of the more recognized members of the group and also one of the most under-recognized in primary care.
A note on terminology before we get into it. The broader medical term has shifted toward "axial spondyloarthritis," or axSpA, which is the umbrella category. Ankylosing spondylitis is now technically a subtype of axSpA, specifically the form with visible structural changes on X-ray. Earlier or milder disease without those X-ray changes is called non-radiographic axSpA. The distinction matters in research and in some treatment decisions, but for the purposes of this post, I'm going to use ankylosing spondylitis throughout, which is how most patients and providers still talk about it.
If you take one thing away from this post, it's this: a young patient with chronic back pain that's worse in the morning and better with movement deserves a workup. That pattern, called inflammatory back pain, is a real clinical entity and it's the most important early clue.
What it is
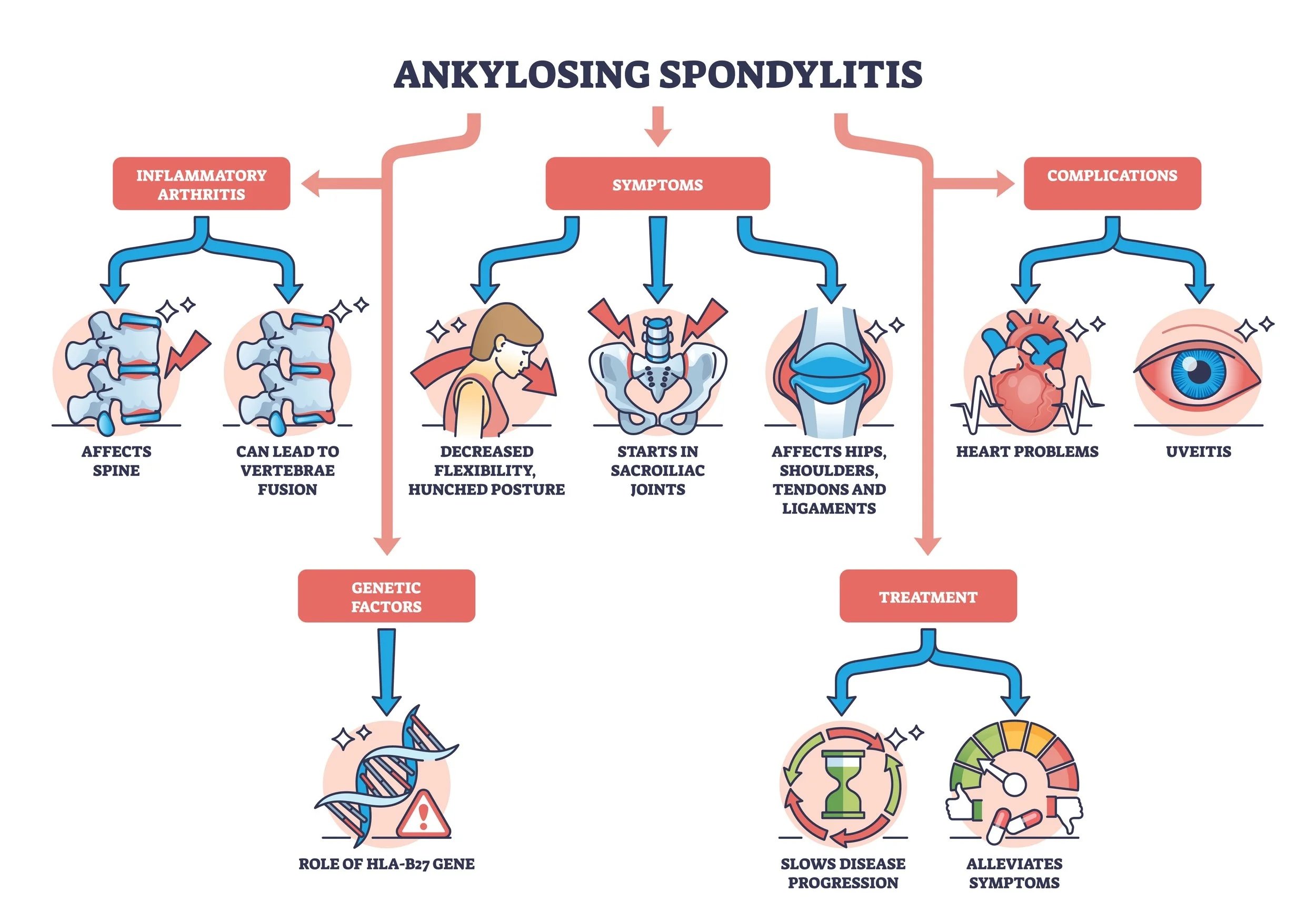
Ankylosing spondylitis is an inflammatory disease that primarily affects the spine and the sacroiliac (SI) joints, the joints where the lower spine meets the pelvis. The inflammation usually starts in the SI joints and over time can migrate up the spine. In long-standing, severe disease, parts of the spine can fuse together, which is where the word "ankylosing" comes from (it means stiffening or fusion).
Symptoms typically start in the 20s or 30s, with most patients developing symptoms before age 45. It's more common in men, although we now recognize that AS in women has historically been underdiagnosed and the actual sex ratio is closer than we once thought.
Inflammatory back pain
The hallmark of AS is inflammatory back pain, which has a specific pattern that differs from mechanical back pain:
It comes on gradually rather than after an injury
It's worse in the morning and after periods of rest
It improves with movement and exercise
Morning stiffness lasts longer than 30 minutes
It often wakes patients up in the second half of the night
It's typically in the low back or buttocks, sometimes alternating sides
Compare this to mechanical back pain, which is generally worse with activity and better with rest. The two patterns behave in opposite directions, which is one of the most useful clinical distinctions in this space.
When a young patient has this pattern of back pain, AS belongs in the differential.
Beyond the back
AS doesn't only affect the spine. Other features that can show up:
Peripheral joint involvement, usually asymmetric and in larger joints like the hips and knees
Enthesitis, particularly at the heels
Uveitis (a particular kind of eye inflammation), which can be a presenting feature
Fatigue, which is often underappreciated
These extra-articular features are part of what links AS to the broader spondyloarthritis family.
HLA-B27
We touched on this in the primer post, but it's worth revisiting in the context of AS specifically.
HLA-B27 is strongly associated with ankylosing spondylitis. Most patients with AS are HLA-B27 positive. But the test is still a piece of the puzzle, not a diagnosis. About 6 to 8% of the general population is HLA-B27 positive, and the vast majority of those people will never develop AS.
What HLA-B27 does is raise the clinical suspicion when the picture fits. A young patient with inflammatory back pain who is HLA-B27 positive has a meaningfully higher probability of AS. The same patient with mechanical low back pain after lifting boxes doesn't change much based on the marker
Diagnosis
AS is a clinical diagnosis. The combination that I'm looking for is:
A young patient with inflammatory back pain
Supportive labs (HLA-B27 status, plus inflammatory markers like ESR and CRP, although these can be normal)
Imaging that supports the diagnosis (MRI of the SI joints, sometimes X-ray)
MRI is the most sensitive imaging tool for early disease, since X-rays often don't show changes until later in the disease course. MRI can pick up active inflammation in the SI joints before structural damage is visible.
There are some important caveats to MRI, though. First, false positives are real. Bone marrow edema in the SI joints can be seen in young athletes, postpartum women, and even healthy individuals. In one study, 30 to 41% of elite athletes and recreational runners had MRI findings that met the imaging criteria for sacroiliitis without having any actual inflammatory disease. Postpartum women had even higher rates. The imaging has to be interpreted in clinical context.
Second, a negative MRI doesn't rule out AS. There are patients with the clinical picture, supportive labs, and a treatment response who never have a clearly positive MRI. In those cases, if the clinical suspicion is high and other supporting features are present, I'll sometimes trial a TNF inhibitor for about three months. If the patient responds, that's meaningful supportive evidence. If they don't, true AS becomes much less likely.
Imaging is a tool. The diagnosis is clinical.
Treatment
Treatment of AS has changed dramatically over the past two decades. The goals are to control inflammation, preserve mobility and posture, and prevent the progressive damage that comes with uncontrolled disease.
A few cornerstones:
Exercise and physical therapy. This is not optional. Regular movement, particularly mobility work and posture-focused exercise, is disease-modifying. Patients who stay active do significantly better long-term.
NSAIDs. Often first-line for symptom control. Some evidence suggests regular NSAID use may slow structural progression.
Biologics. TNF inhibitors and IL-17 inhibitors are highly effective in AS. JAK inhibitors are also approved. Notably, methotrexate and other traditional DMARDs are not effective for the axial disease in AS, which is one of the meaningful differences from other spondyloarthritis subtypes like PsA.
I'll go deeper on the medication classes in future posts..
The bottom line
Young patient. Chronic back pain. Worse in the morning, better with movement. That pattern is worth a workup.
AS is treatable, and early treatment matters. The diagnostic delay in AS has historically been measured in years, and that delay translates into preventable structural damage. The faster we identify it, the better we can protect the spine.
References
Sacroiliitis on MRI: axSpA or Another Cause? The Rheumatologist, 2024. https://www.the-rheumatologist.org/article/sacroiliitis-on-mri-axspa-or-another-cause/
Kiltz U, et al. Non-Radiographic Axial Spondyloarthritis. Current Rheumatology Reports, 2016. https://pubmed.ncbi.nlm.nih.gov/26897981/
Magrey MN, et al. Recognizing Axial Spondyloarthritis: A Guide for Primary Care. Mayo Clinic Proceedings, 2020. https://www.mayoclinicproceedings.org/article/S0025-6196(20)30153-1/fulltext