
The SetPoint System for Rheumatoid Arthritis: A Rheumatologist’s Review

A quick disclosure before we start: I don’t implant this device, I don’t sell it, and I have no financial relationship with the company.
I met with their team simply because I wanted to understand the device better, get a handle on the practical side (how a patient actually gets one), and see if anyone in our area is performing the surgery yet. Here is what I found.
In July 2025, the FDA approved something entirely new for rheumatoid arthritis. Not a new drug, but a device.
It’s called the SetPoint System. It is a small implant placed directly on the vagus nerve on the left side of your neck.
Here is what living with it actually looks like:
The Procedure: Outpatient surgery under general anesthesia using a single incision to place the implant.
Daily Use: One minute of nerve stimulation per day, usually while you sleep.
Maintenance: Charge it with a collar for about 10 minutes a week. Battery lasts around 10 years.
This is the first approved treatment for RA that isn’t a medication. Patients have been asking me about it since the news broke, so let’s get into it.
How It Works: Pressing the Body's Natural Brake
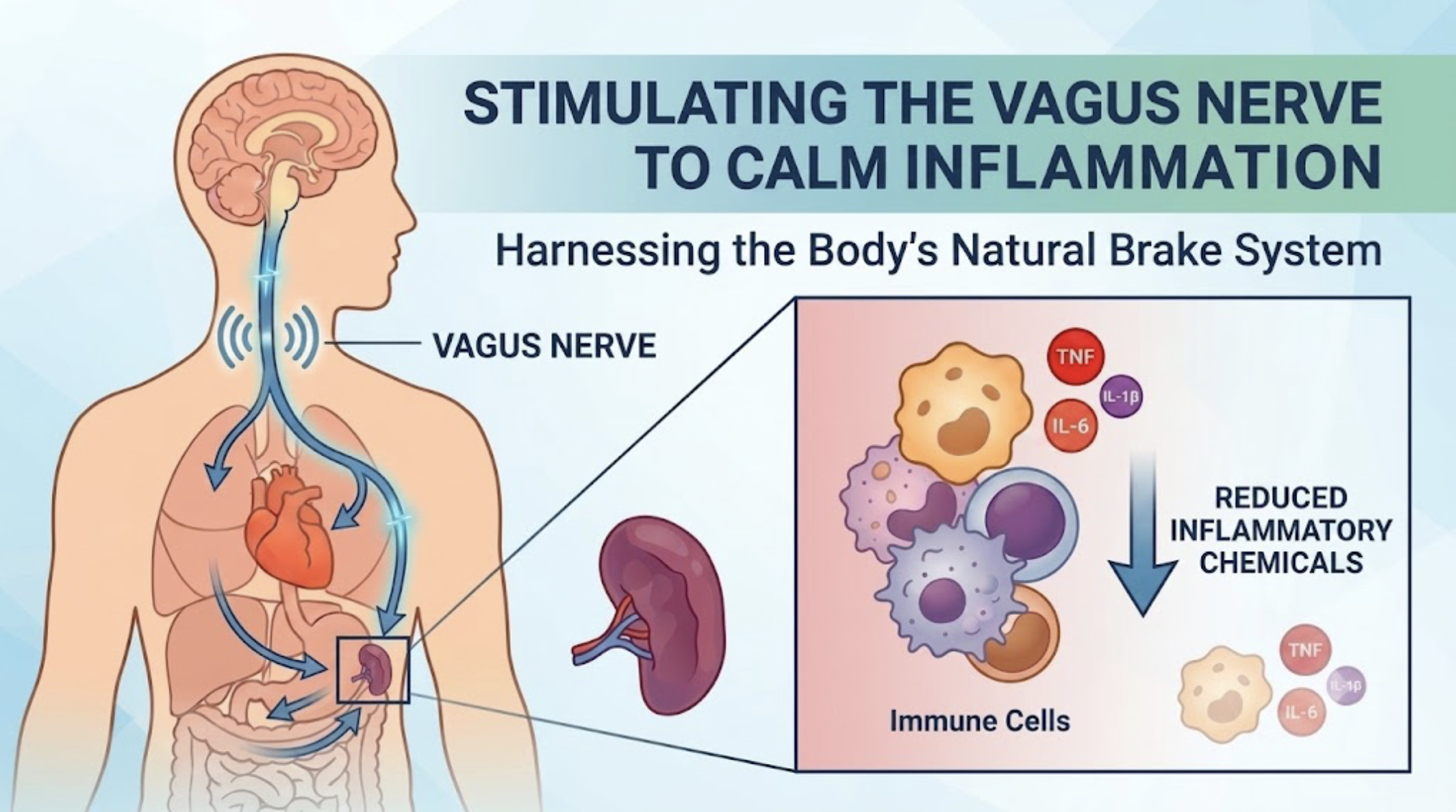
Simplified diagram of vagus nerve stimulation effect on the immune system.
Your body has a built-in brake on inflammation, and it runs right through the vagus nerve. When active, it tells immune cells to produce fewer of the inflammatory chemicals (TNF, IL-6, and others) that drive RA — the exact same chemicals that our biologic medications block.
In people with RA, that natural brake tends to run weak. This implant is an attempt to press down on that brake.
What the Study Showed
The RESET-RA trial enrolled 242 patients with moderate to severe RA who had failed at least one biologic or JAK inhibitor. Everyone got the implant. Half were switched on, half left off — and nobody knew who was who. A true gold-standard surgical trial.
Important to remember: the device was always used on top of methotrexate or similar medications. These results reflect the combination, not the device alone:
At 3 months (blinded):
Device ON: 35.2% achieved ACR20 response (a 20% improvement in symptoms)
Device OFF: 24.2% achieved ACR20
This initial gap is real, but modest. To compare, biologic drugs in similar patients typically hit ACR20 rates of 50-70%.
At 6-12 months (unblinded — everyone’s device turned on)
Response climbed to around 50%
Encouraging, but when people know they are getting the real treatment, results tend to look better.
Other key findings:
At 12 months: 75% had not needed to add a biologic back, though that doesn’t always mean disease was well-controlled. Looking forward to seeing longer term data on this in the future.
The device worked best in patients who had failed only one biologic (44.2% vs 19% sham). Smaller subgroup, so less reliable but still notable.
One important point: The device and medication are not mutually exclusive. If your disease flares, you can still add a biologic or JAK inhibitor. Getting the implant doesn’t mean giving up other treatments.
What Can Go Wrong
The serious adverse event rate was 1.6%. All 4 patients recovered. But the risk profile is completely different from daily medication. It’s front-loaded and surgical, not ongoing.
Your Voice - The biggest thing to understand:
The vagus nerve runs right alongside the nerve that controls your vocal cords.
About 1 in 14 patients had hoarseness after surgery. Most improved within months; a few took up to a year or needed speech therapy.
Bottom line: If you use your voice for your livelihood (teaching, sales, singing), this deserves a careful conversation.
Surgical Risks: Swelling, soreness, and minor infection at the incision site (standard surgical stuff). Some patients felt mild discomfort from the stimulation itself, which was usually fixed by adjusting the settings downward.
What Wasn't There: Through a full year of tracking, there were no serious infections, no cancers, no heart attacks, and no blood clots. That said, 242 patients for one year is a small safety dataset.
If you take a biologic or a JAK inhibitor, you know that list well. It’s why we run regular labs and hold your medications when you’re sick. This device doesn’t carry that baggage. You take the surgical risk on once, and then it is behind you.
Who is it for - and Where it Fits
Approved for: Adults with moderate-to-severe RA who have failed, lost response to, or couldn't tolerate at least one biologic or JAK inhibitor. You do not have to have run out of drug options to qualify - failing one is enough.
You cannot get it if you have:
An implanted pacemaker or defibrillator (the chargers can interfere with each other).
A prior vagotomy (cut vagus nerve) or splenectomy (removed spleen), as the device requires both to be intact to work.
An inability to safely undergo general anesthesia.
Lifestyle notes: MRIs require special protocols and a two-week wait after implant. No scuba diving or hyperbaric chambers (device hasn’t been tested under those extreme pressures).
Where I think it fits best: The question isn’t how many drugs you’ve failed - it’s whether you can safely take immunosuppression at all. I’m thinking of:
Patients with active or recent cancer
Patients with recurrent, severe infections
Patients with demyelinating diseases like MS
Patients who get severe side effects from nearly every medication
People who simply don’t want to be on chronic medication.
For these patients, a treatment with proven efficacy and without the same immunosuppression risks is a big win.
Insurance coverage is still an open question. The device is a one-time cost vs. the ongoing expense of biologics, but we don’t yet have formal comparisons.
What About the Drugstore Versions?
You can buy non-surgical vagus nerve stimulators online. To be clear, none of these over-the-counter versions have been proven to work for RA.
Ear Clips: Tested in a controlled trial of 113 RA patients. No difference from a fake device.
Handheld Neck Devices: Tiny studies, no control group. Can’t separate real results from placebo.
Deep Breathing: Naturally increases vagal activity. No formal RA studies, but it’s free, takes 10 minutes, and has real mental health benefits. I recommend it regardless.
Where Things Stand
Availability: Currently available in Minnesota at a limited number of sites, with more opening soon.
What’s next: Trials are underway for a wearable ultrasound version that stimulates the spleen. No surgery, no implant. The U of Minnesota is one of the trial sites.
My Take: This is a single trial, and the strongest data only covers 3 months. But the safety profile is unlike anything else we have for RA. For patients who struggle with medication side effects or want to avoid immunosuppression, this is worth discussing.
As my patients begin using this technology, I’ll update this blog with what we see in the real world.
If you are wondering whether this approach makes sense for your RA, this is exactly the kind of nuance we can map out together at a visit.
Have a question you want answered? Schedule a free virtual meet and greet, or email me at drmiller@restorerheumatology.com.
Sources
The main trial (RESET-RA): Tesser JRP, et al. "Vagus nerve-mediated neuroimmune modulation for rheumatoid arthritis: a pivotal randomized controlled trial." Nature Medicine, 2026.
FDA approval and device information: SetPoint System, FDA (PMA P240039), 2025; SetPoint System Prescriber Instructions for Use.
Tocilizumab comparison (RADIATE): Emery P, et al. Annals of the Rheumatic Diseases, 2008.
Abatacept comparison (ATTAIN): Genovese MC, et al. New England Journal of Medicine, 2005.
Ear-device trial (auricular VNS): Baker MC, et al. Arthritis & Rheumatology, 2023.
Neck-device study (non-invasive cervical VNS): Marsal S, et al. Lancet Rheumatology, 2021.
Spleen ultrasound trial at the University of Minnesota: SecondWave Systems ULTRA study, ClinicalTrials.gov NCT07163221.